Skip to content
Home
About Us
Pipeline Products
Kinostat®
Nutraceutical Antioxidants
MFRMS
Our Services
For Investors
Publications
Contact Us
×
Home
About Us
Pipeline Products
Kinostat®
Nutraceutical Antioxidants
MFRMS
Our Services
For Investors
Publications
Contact Us
Home
About Us
Pipeline Products
Kinostat®
Nutraceutical Antioxidants
MFRMS
Our Services
For Investors
Publications
Contact Us
×
Home
About Us
Pipeline Products
Kinostat®
Nutraceutical Antioxidants
MFRMS
Our Services
For Investors
Publications
Contact Us
Search
Search
Close
Search
Search
Close
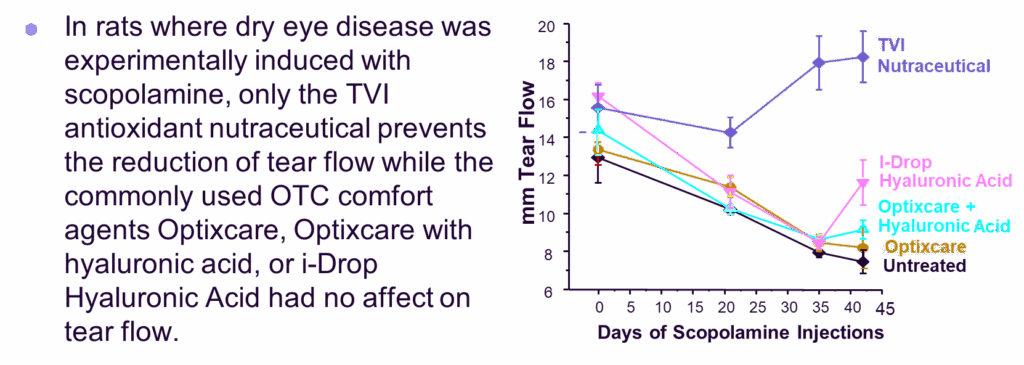
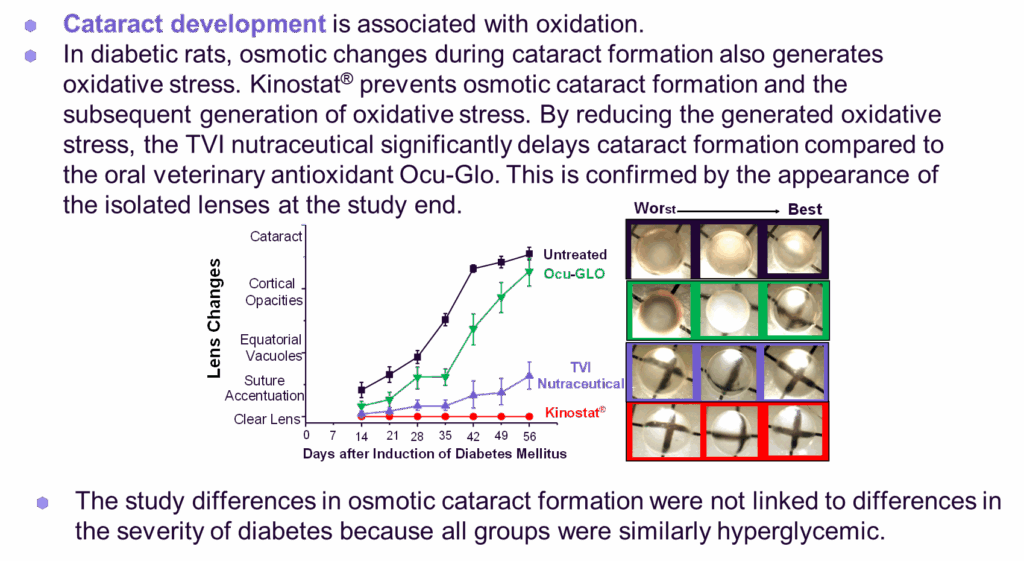
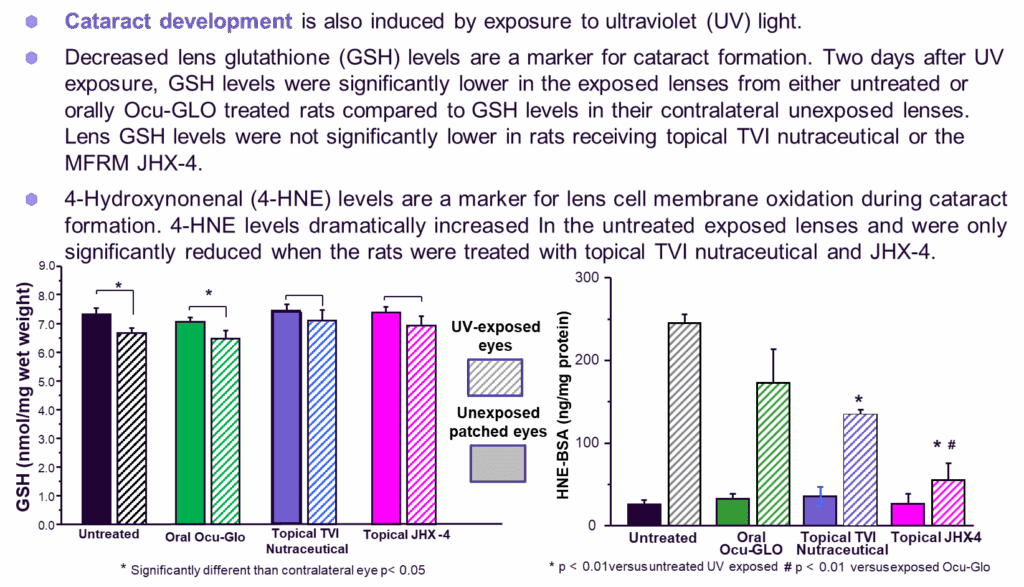
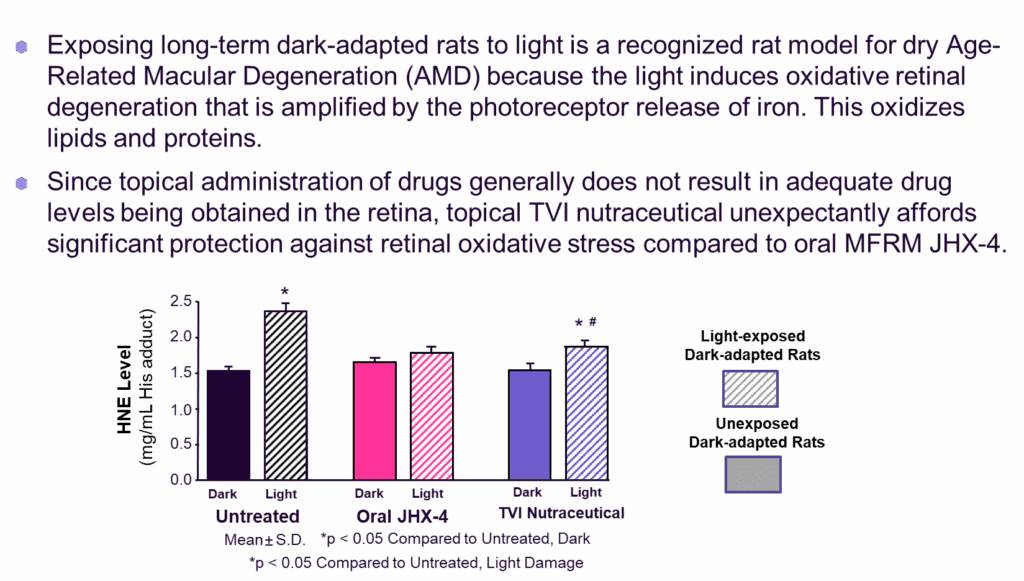
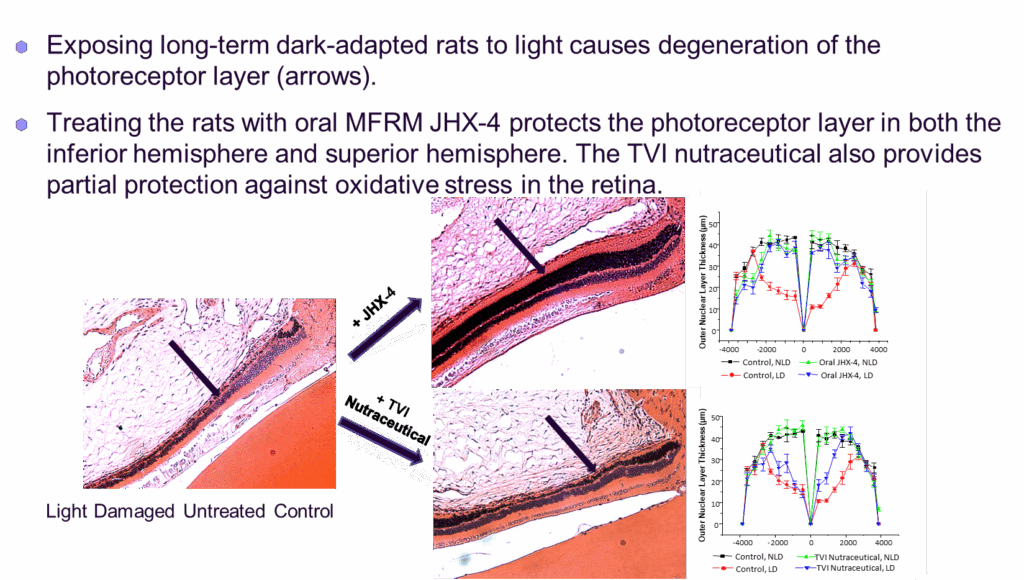
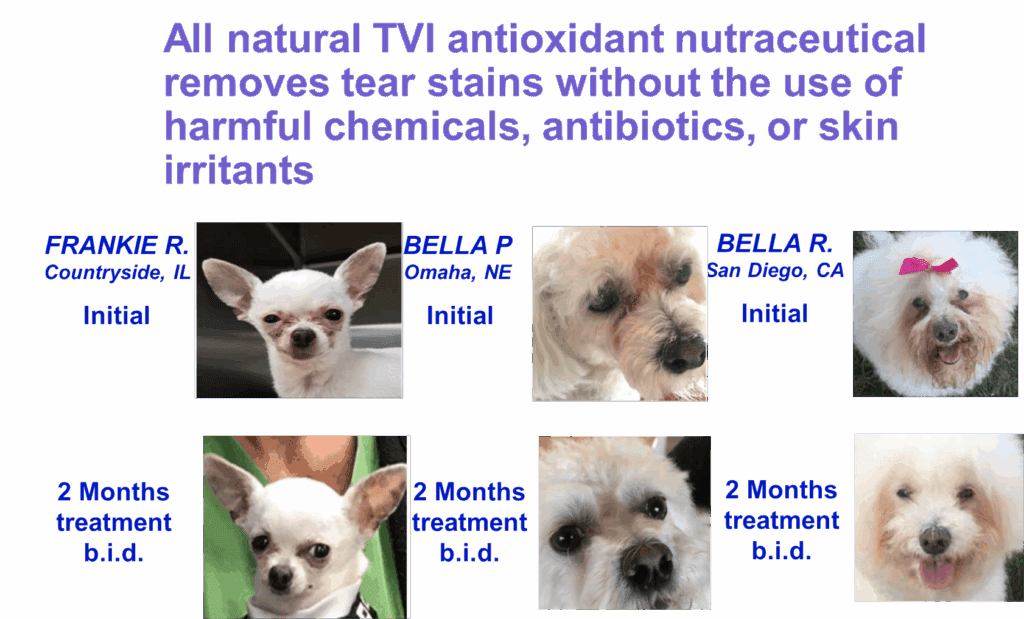
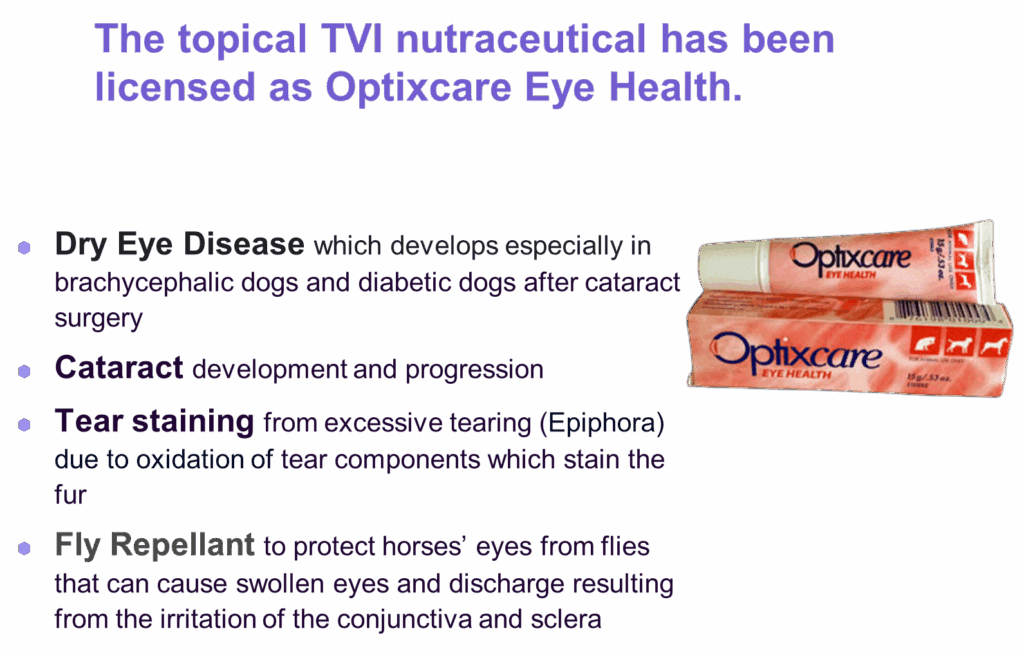
Topical Applied Nutraceutical Antioxidant Formulation Reduces Ocular Oxidative Stress (press title)
Nutraceutical Antioxidant
Posts navigation
← What is Diabetic Keratopathy and Its Treatment?
What are Redox Reactions and Why is Redox Modulation So Important? (press title) →
Scroll To Top